Investigating Wrestling Injuries
Enrico N. Esposito, Chair of Sports Medicine, United States Sports Academy, USA.
Introduction
Grindstaff & Potach (2006) showed that wrestling is one of the oldest sports in the world, with its roots embedded in the first Olympic Games in 776 B.C. Wrestling , both a contact and collision sport, places extreme demands on the entire body and much demands all too often result injury. Two common styles of wrestling exist in the FILA (International Federation of Associated Wrestling Styles): freestyle, and Grexo-Roman, all with a common goal of pinning the opponent. It is a highly anaerobic sport, requiring maximal power and strength for explosive attacks during each mach. Wrestling match may last up to 10 minutes in the official competition (Kraemer et al.,2001; Grindstaff, & Potach, 2005).
Many wrestlers are inexperienced, especially at the middle- and high-school levels, and thus close attention to proper technique is essential for a safe competition. (Hewett et al.,2005). Obviously, the development of these metabolic systems plays a key role in the wrestling’s success Kraemer et al.,2001; Lansky et al.,1999). Most of the physiological changes were thought to be related to rapid weight loss methods and inadequate recovery between matches (Kraemer et al.,2001;Webster et al.,1990).
Injury and Injury Prevention
Strength and condition professionals must understand not only injuries common to wrestling but also how a properly design, well-planned strength training and conditioning program may help to decease this high injury rate and reduce the risk of common injuries while improving performance (Grindstaff, & Potach, 2006). During the 2003-2004 academic year, per 1,000 athlete exposures, 5.7 injuries during practice and 25.8 injuries during matches occurred. Both ranked second behind spring football practice and football games (Athletic,2004). High school wrestling holds a comparable injury rate of 6.0injuries per 1.000 exposures (Pasque et al.,2000). At both the collegiate and high school levels, most injuries occur in the neutral position during take down type activities (Boden et al., 2002; Jarret et al., 2004; NCAA et al., 2004; PASQUE et al., 2000). Common injury sites are the knee, face, shoulder, ankle, and neck (Jarret et al., 2004; Ncaa et al. ,2004; Pasque et al., 2000). Most injuries occur as a result of contact with a competitor or mat or twisting forces (Ncaa et al. ,2004; Pasque et al., 2000). It is thought that injury prevention programs develop an individual’s ability to decrease landing forces.
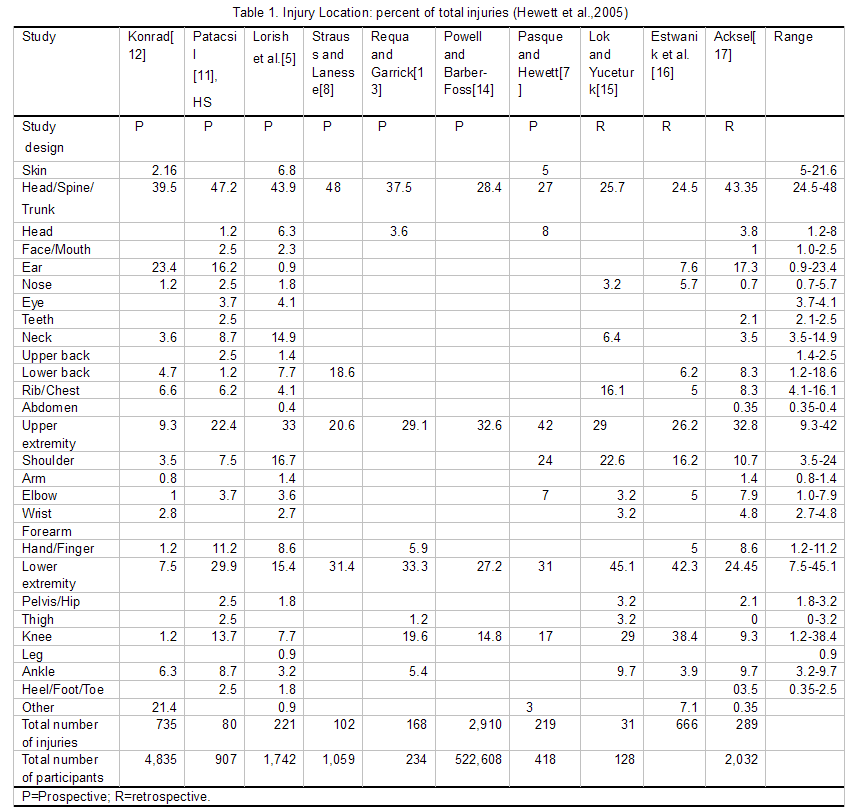
Review of this table reveals that the body region incurring the greatest percentage of injuries is the head/spine/trunk (range of 24.5–48%) followed by the upper extremity (range of 9.3–42%). The next highest is the lower extremity (range of 7.5–45.1%) and lastly the skin (range of 5–21.6%) (Lorish et al, 1992; Pasque, & Hewett,2000; Strauss,1982; Patacsil,1955; Konrad, 1951; Requa, & Garrick, 1981; Powell, 1999; Lok,& Yuceturk, 1974; Estwanik, 1980; Acksel, 1966). Concussions and other head injuries have occurred from 1–8% of all wrestling injuries (Table 1). (Lorish et al, 1992; Pasque, & Hewett,2000; Patacsil,1955). However, Hewett, Pasque, Heyl, & Wroble (2005) found that several potential areas for decreasing injury risk in wrestlers, including equipment, coaching, officiating and training. However, informed decisions with regard to preventing injuries are dependent upon the quality of the basic epidemiological data available, and at this time, analyses of risk factors and potential preventive measures are lacking.
A study examining high school wrest ling injuries mated that wrestlers with general ligament us laxity suffered fewer shoulder injuries than did the other wrestlers (Pasque et al., 2000). Therefore, shoulder flexibility should be an essential component of injury prevention programs. In addition to flexibility, rotator cuff strength, endurance, shoulder stability, and proper muscle balance should be addressed. Wrestling-specific exercises for the shoulder should involve both weight bearing and non-weight-bearing positions. Weight-bearing exercises, such as push-up variations. Produce muscle co-contraction, resulting in creased joint stabilization and proprioception (Rogoi et al., 1998; Ubinger et al., 1999; Uhl et al., 2003). Plyomrtric exercises should also be incorporated to increase shoulder strength, power, and proprioception. Most relevant studies have related serious wrestling injuries to the head and face: contusion, laceration, facial fracture, dislocation, and concussion (Koh et al., 2002; Pieter et al., 1998; Siana et al.,1986; Koh et al.,2001).
Therefore, injury prevention, A wrestling match takes place on a slightly unstable surface (i.e., a cushioned mat). Additionally, match situations may require single limb stance or that the athletes support some of their body weight with 1 or 2 hands for a prolonged period. Because of these precarious positions and unstable environments, with previous joint injury only compounding this risk (Buss et al., 2004; Jones et al., 1993; Kraemer et al., 2002; Mugrom et al.,1991; Surve et al., 1994; Tropp et al.,1985; Verhagen et al.,2004). Additionally, individuals with decreased strength, balance, proprioception, and neuromuscular control are also at greater risk for injury (Hewett et al., 2005; Leetun et al., 2004; Whiems et al., 2005).
Summary
Better attention by wrestling officials to rules infractions and dangerous moves can also be crucial in preventing serious injury (Hewett et al.,2005). Wroble(1996) discussed beginning practices earlier in the season, and delaying the onset of competition to allow for wrestlers to be better prepared for competition. Pasque and Hewett(2000) showed suggest that limiting the amount of time spent practicing live wrestling may decrease the incidence of injuries occurring during practice.
Boden et al. (2002) found that coaches teach wrestlers to keep their heads up when performing shooting or takedowns, to avoid axial compression or flexion of the spine leading to serious injury. Coaches should always help educate the athletes in preventing from sport injuries, particularly during the extremely competitive matches, wherein permanent injuries or even fatal consequences are likely incurred (Pieter et al., 1998).
References
Athletic(2004). NCAA Men’s Wrestling Injury Surveillance System for Academic Year 2003-2004. Indianapolis: National Collegiate. Athletic Association.
Acksel, J.(1966). A study of interscholastic wrestling injuries in the state of Missouri during the 1965–1966 season. Eastern Illinois University.
Boden, B.P., Lin, W., Young, M., & Mueller, F.O.(2002). Catastrophic injuries in wrestlers. Am J Sports Med, 30, 791–795.
Buss, D.D., Lynch, G.P., Meyer, C.P., Huber, S.M., & Freehll, M.Q. (2004). Nonoperative management for in-sea-son athletes with anterior shoulder in-stability. Am.J.Sports Med. 32:1430-1433.
Estwanik, J.J., Bergfeld, J.A., & Collins, H.R. et al(1980). Injuries in interscholastic wrestling. Physician Sportsmed ,8 , 111–121.
Grindstaff, T.L., & Potach, D.H.(2006). Prevention of Common Wrestling Injuries. Strength and Conditioning Journal, 28(4), 20-28.
Hewett, T.E., Pasque, C., Heyl, R., & Wroble, R. (2005). Wrestling Injuries. Med Sport Sci. 48, 152-178.
Hewett, T.E., Myer, G.D., Ford, K.R., Heidt, R.S., Colosimo, A.J., Mclean, S.G., Van Den Bogert, A.J., Paterno, M.V., & Succop, P.(2005). Biomechanical measures of neuromuscular control andvalgus loading of the knee predict anterior cruciate ligament injury risk in female athletes. Am. J. Sports Med.33:492-501.
Jones, B.H., Cowan, D.N., Tom-Linson, J.P., Robinson, J.R., Polly, D.W., & Frykman, P.N.(1993). Epidemiology of injuries associated with physical train-ing among young men in the army. Med.Sci.Sports Exerc.25:197-203.
Konrad, I.(1951).A study of wrestling injuries in high schools throughout seven midwest states. Michigan State College.
Koh, J.O., DeFreitas, T., & Watkinson, E.J. (2001): Injuries at the 14th World Taekwondo Championships in 1999. International Journal Apply Sports Science, 13:33-48.
Koh, J.O., & Watkinson, E.J. (2002): Video analysis of blows to the head and face at the 1999 World Taekwondo Championships. J Sports Med Phys Fitness, 42(3):348-354.
Kraemer, W.J., Fry, A.C., Rubin, M.R., Triplett-Mcbride, T., Goridon, S.E., Koziris, L.P., Lynch, J.M., Volek, J.S., Meuffels, D.E., Newton, R.U., & Fleck, S.J. (2001). Physiological and performance response to tournament wrestling. Med Sci. Sports Exerc. 33:1367-1378.
Kraemer, F.S., Goiser, K., Wis-Chatta, R., Wambacher, M., & Sperner, G.(2002). Predicting recurrence after primary anterior shoulder dislocation. Am. J. Sports Med. 30:116-120.
Lansky, R.C.(1999). Wrestling and Olympicstyle lifts; In-season maintenance of power and anaerobic endurance. Strength. Cond. J. 21:21-27.
Lok, V., & Yuceturk, G.(1974). Injuries of wrestling. J Sports Med, 2, 324–328.
Leetun, D.T., Ireland, M.L., Willson, J.D., Ballantyne, B.T., & Davis, I.M.,(2004).Core stability measures as risk factors for lower extremity injury in athletes.Med. Sci. Sports Exerc. 36:926-934.
Lorish, T.R., Rizzo, T.D., Ilstrup, D.M., & Scott, S.G.(1992). Injuries in adolescent and preadolescent boys at two large wrestling tournaments. Am J Sports Med ,20, 199–202.
Mugrom, C., Shlamkovttch, N., Finestone, A., Eldad, A., Laor, A., Danon, Y.I., Lavif, O., Wosk, J., & Simkin, A.(1991). Risk factors for lateral ankle sprain:A prospective study among military recruies. Foot. Ankle. 12:26-30.
Ncca(2004):Men’s Wrestling Injury Surveillance System for Academic Year 2003-2004. Indianapolis: National Collegiate. Athletic Association.
Pasque, C.B.,& Hewett, T.E(2000). A prospective study of high school wrestling injuries. Am J Sports Med,28, 509-515.
Patacsil, J.(1955). An analytical survey of the incidents of injuries sustained in intercollegiate and interscholastic wrestling. West Lafayette, Purdue University.
Pieter, W., & Zemper, E.D. (1998) : Incidence of reported cerebral concussion adult Taekwondo athletes. Journal Roy Soc Health, 118:272-279.
Powell, J.W., & Barber, K.D.(1999). Traumatic brain injury in high school athletes. JAMA ,282, 958-963.
Requa, R., & Garrick, J.(1981). Injuries in interscholastic wrestling. Physician Sportsmed, 9 , 44–51.
Rogoi, I.M., Ernst, G., & Perrin, D.H.(1998). Open and closed kinetic chain exercise improve shoulder joint reposition sense equally in healthy subjects. J. Atbl. Train. 33:315-318.
Strauss, R.H., & Lanese, R.R.(1982).Injuries among wrestlers in school and college tournaments. JAMA, 248,
Siana, J.E., Borum, P., & Kryger, H. (1986): Injuries in Taekwondo. J Sports Med,
20:165-466.
Surve, I., Schwellnes, M.P., Noakes, T., & Lombard, C.(1994). A. fivefold reduction in the incidence of recurrent ankle sprains in soccer players using the sport-stirrup orthosis. Am.J.Sports Med. 22:601-606.
Tropp, H., Askling, C., & Guqutst, J.(1985). Prevention of ankle sprains. Am.J.Sports Med. 13:259-262.
Ubinger, M.E., Prentice, W.E., Guskiewicz, K.M., & Schneider, R.(1999). Effect of closed kinetic chain training on neuromuscular control in the upper extremity. J. Sport Rebabil. 8:187-194.
Uhl, T.L., Carver, T.J., Mattacola, C.G., Mair., S.D., & Nitz, A.J.(2003). Shoulder musculature activation during upper extremity weight-bering exercise. J. Ortbop. Sports Pber. 33:109-117.
Verhagen, E., Van Der Befk, A., Twisk, J., Bouter, L., Bahr, R., & Van Mechelen, W.(2004). The effect of a proprioceptive balance board training program for the prevention of ankle sprains: A prospective controlled train. Am. J. Sports Med. 32:1385-1393.
Whiems, T.M., Whvrouw, E., Dhbafre, K., Mahifc, N., De Bocrdeaudhuij, I., & Chrco, D.DE.(2005). Intrinsic risk factors for inversion ankle sprains in male subjects: A prospective study. Am. J. Sports Med. 33:415-423.
Wroble, R.(1996). Wrestling. Epidemiology of sports injuries. Champaign, Human Kinetics.